
Understanding the mental health landscape for LGBTQ+ youth
Addressing the Mental Health Needs of LGBTQ+ Youth: A Practical Guide for Families, Educators, and Clinicians
Providing affirming, evidence-based mental health support for LGBTQ+ youth requires coordinated effort across homes, schools, and clinical settings. This guide synthesizes current research, practical strategies, and vetted resources so families, teachers, and clinicians can act with confidence and compassion.
Defining terms and scope: who we mean by LGBTQ+ youth
“LGBTQ+ youth” refers to young people who identify as lesbian, gay, bisexual, transgender, queer/questioning, plus identities such as nonbinary, genderfluid, intersex, Two‑Spirit, and other sexual orientations and gender identities. In practice, the term covers adolescents and young adults roughly ages 12–24, though resources and legal consent rules vary by jurisdiction.
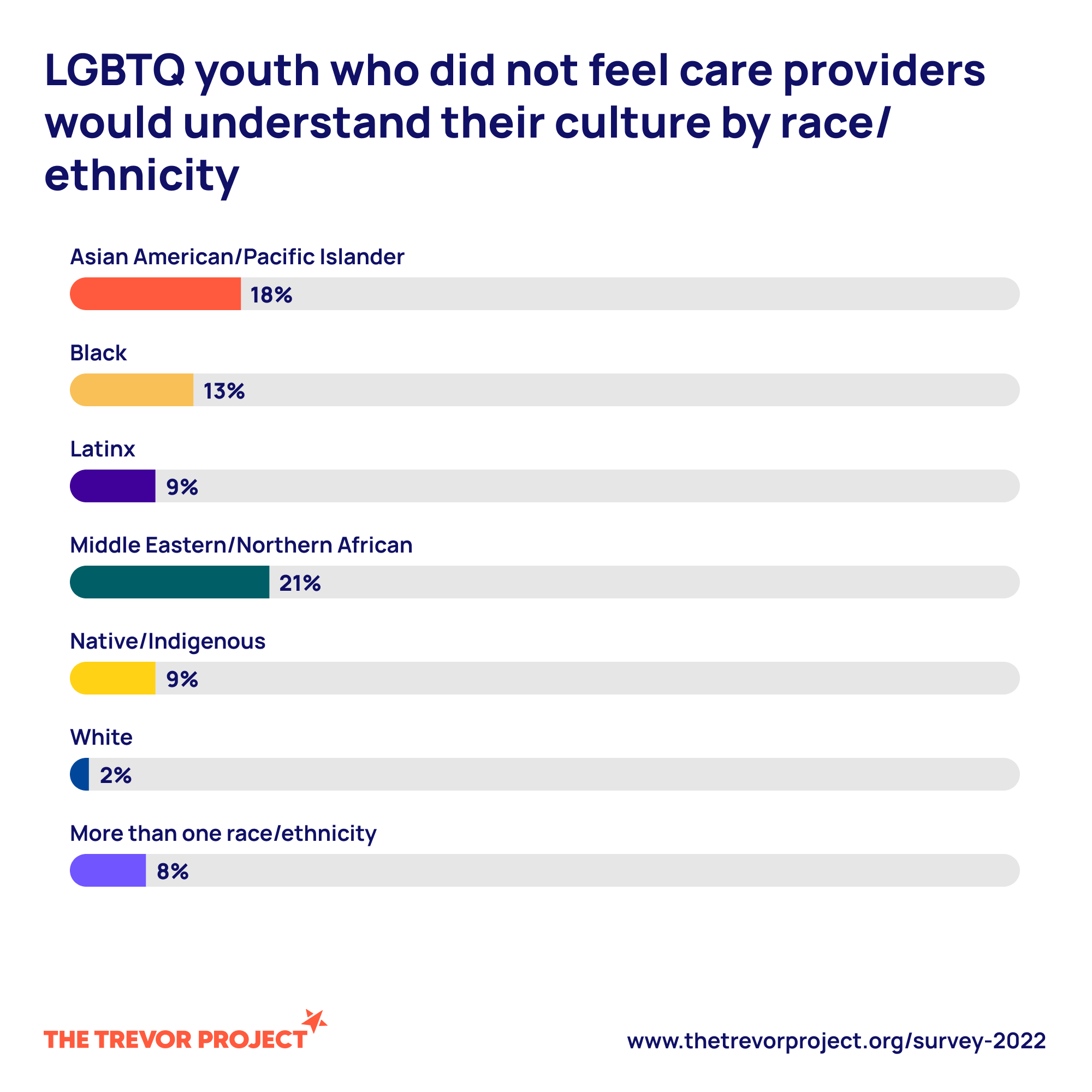
- Intersectionality matters: race, ethnicity, disability, immigration status, socioeconomics, and religion shape experiences and access to care. Youth who hold multiple marginalized identities often face compounded stressors and disparities.
- Terminology evolves; use the language youth prefer and ask respectfully when unsure.
Key trends and statistics on LGBTQ+ youth mental health challenges
LGBTQ+ youth experience disproportionately high rates of mental health concerns compared with their cisgender, heterosexual peers.
- Depression and anxiety: Studies show elevated rates of depressive symptoms and anxiety among sexual and gender minority youth. For example, The Trevor Project 2023 National Survey found high rates of depressive symptoms and anxiety among LGBTQ+ young people. (See The Trevor Project resources below.)
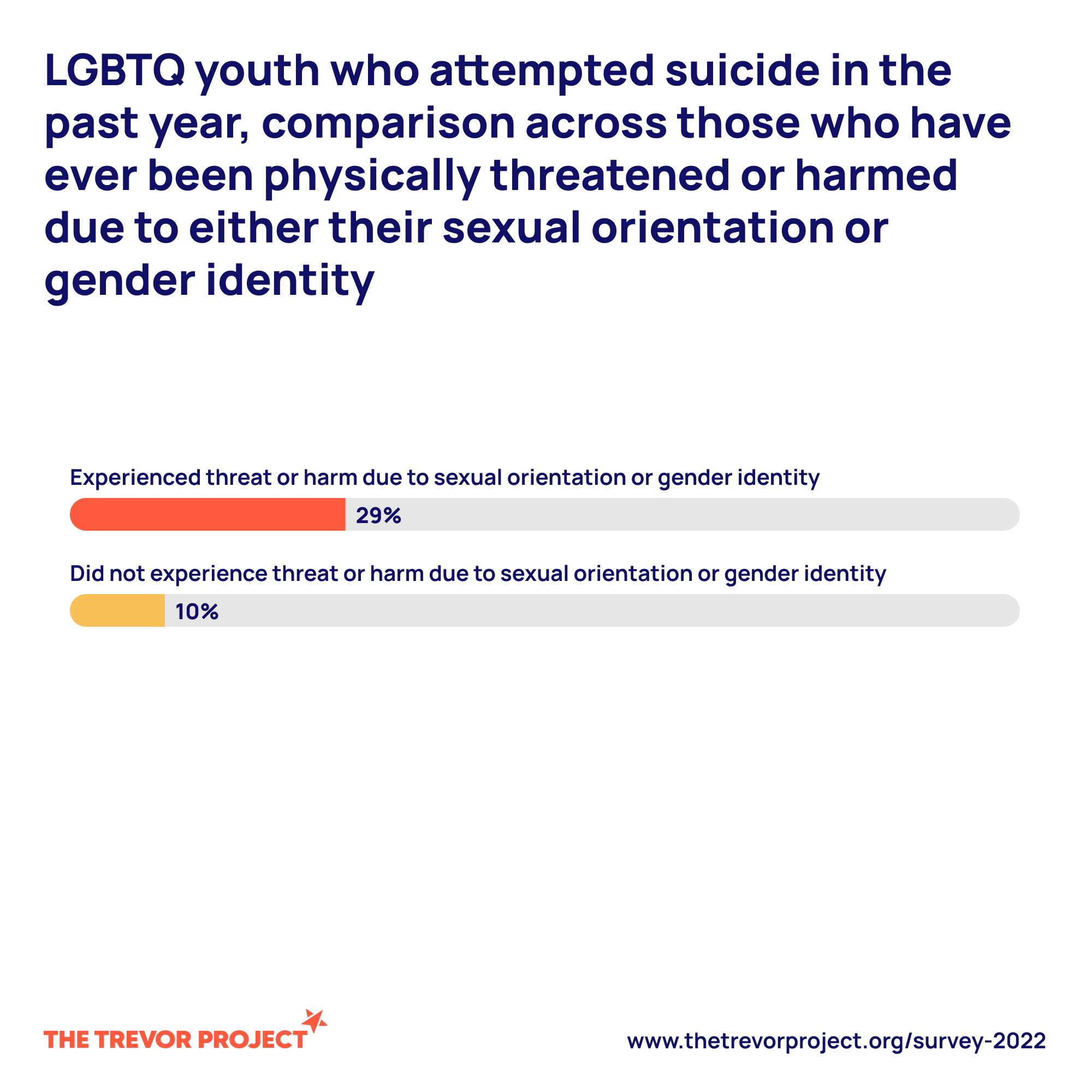
- Suicidal ideation and attempts: LGBTQ+ youth report higher lifetime and recent suicidal ideation and attempts — a consistent finding across national surveys.
- Substance use: Substance use patterns can be increased as a coping mechanism for minority stress and trauma.
Why these disparities occur:
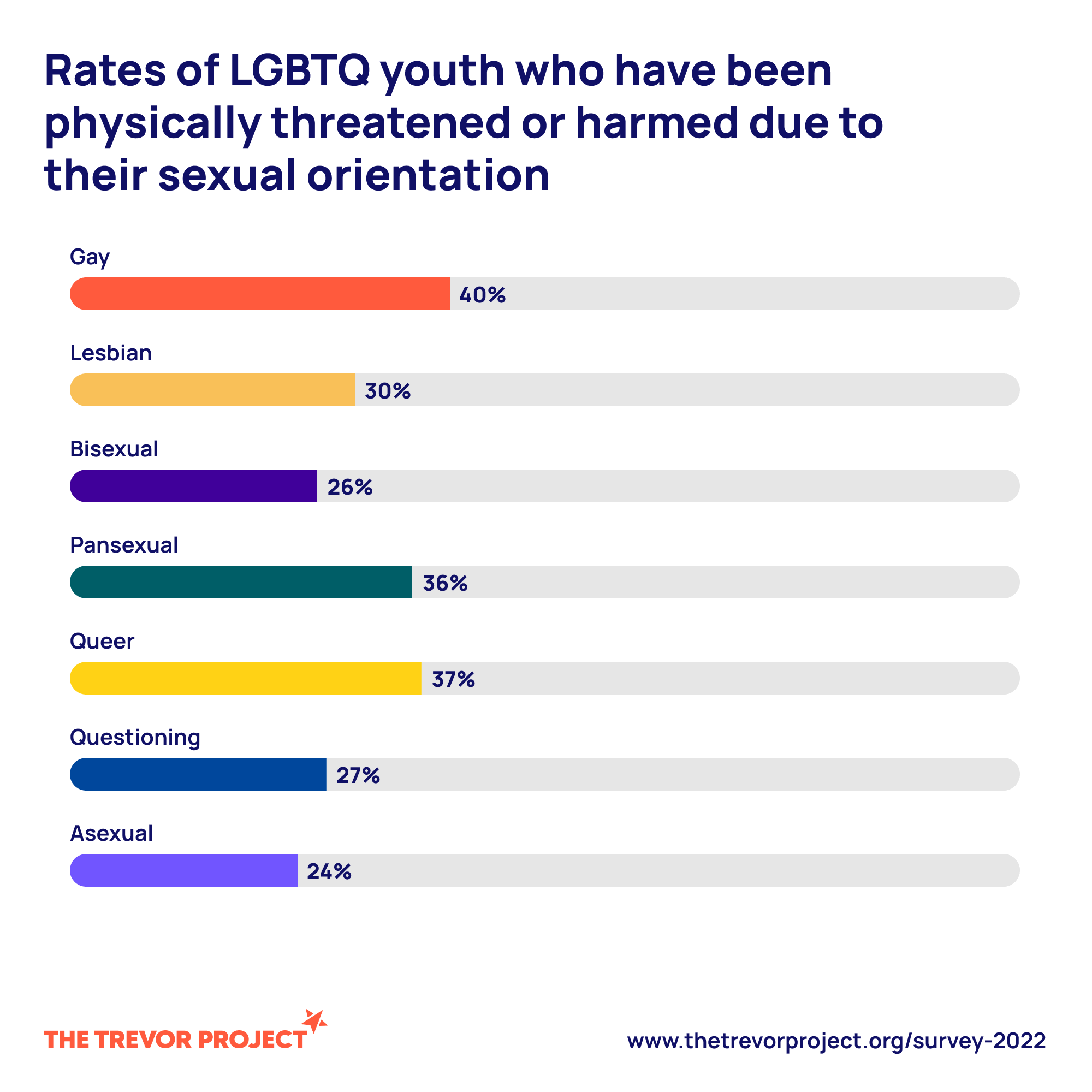
- Discrimination, stigma, and minority stress — ongoing external and internalized stressors linked to identity — significantly increase risk.
- Victimization and bullying at school or in the community create trauma exposures that worsen outcomes.
- Family rejection is a strong predictor of poor mental health and increased suicide risk.
(For reliable statistics, see The Trevor Project, CDC Youth Risk Behavior Surveillance, and peer‑reviewed meta‑analyses.)
Barriers to care and disparities in access
- Systemic obstacles: lack of insurance, absence of culturally competent providers, and geographic deserts for LGBTQ+ competent care (especially in rural areas).
- Legal and policy barriers: age‑based consent laws, restrictive policies toward gender-affirming care in some regions, and inconsistent privacy protections.
- Cultural/family-level barriers: stigma within families or faith communities can limit help‑seeking; language barriers and lack of culturally responsive services further impede access.
- Clinic‑level barriers: intake forms, waiting rooms, and intake staff that are not affirming can send subtle messages of exclusion.
Transition: Understanding these challenges points us to therapeutic approaches and system‑level strategies that reduce harm and promote resilience.
Evidence-based therapeutic approaches for LGBTQ+ youth
Affirmative therapy and best practices
Affirmative therapy is an approach that validates and supports LGBTQ+ identities as part of the therapeutic process rather than treating them as pathology.
Core principles:
- Respect and validation of identity and lived experience.
- Gender‑affirming language and correct pronoun use.
- Attention to minority stress and social determinants of health.
- Integration of identity into treatment goals rather than avoidance.
Benefits: Research shows affirmative approaches improve engagement, reduce internalized stigma, and can lower depressive symptoms and suicidality risk when combined with broader supports.
Practical tips for clinicians and allies:
- Update intake forms to include preferred name and pronouns.
- Use gender‑neutral language; correct mistakes and apologize briefly without making the conversation about the provider.
- Seek ongoing training and supervision in LGBTQ+ affirmative care.
Cognitive‑behavioral and trauma‑informed interventions
Evidence‑based therapies such as CBT and trauma‑informed modalities can be adapted for LGBTQ+ youth.
CBT adaptations:
- Address identity‑related negative core beliefs (e.g., “I don’t belong”) alongside standard cognitive restructuring.
- Use behavioral activation to counter social withdrawal.
- Integrate minority stress psychoeducation so youth understand social context for their distress.
Trauma‑informed care:
- Recognize the prevalence of victimization (bullying, assault, family rejection) and avoid re‑traumatization.
- Prioritize safety, choice, collaboration, trustworthiness, and empowerment.
- Screen for PTSD symptoms and adapt exposure work carefully when experiences involve identity‑based violence.
Dialectical behavior therapy (DBT) skills and acceptance‑based strategies can help with emotion regulation and crisis coping.
Family‑focused and community interventions
- Family acceptance interventions: Programs modeled on the Family Acceptance Project teach caregivers to support their child through education, communication skills, and re‑building trust. Family support is among the strongest protective factors for youth wellbeing.
- Multi‑family groups and family therapy approaches can reduce conflict and improve outcomes.
- Peer and community supports: group therapy, peer mentoring, and community centers provide social connectedness and role models that strengthen resilience.
Transition: Schools and community spaces are often the frontline environment for prevention and early support.
Creating safe spaces for LGBTQ+ teens in schools and communities
Policies, training, and school‑based mental health support
- Implement clear anti‑bullying policies that explicitly protect sexual orientation and gender identity/expression.
- Train teachers, counselors, and staff in trauma‑informed, gender‑affirming responses.
- Strengthen school‑based mental health: on‑site counselors, referral pathways to LGBTQ+ competent clinicians, and routine screening for mood and suicidality.
Example programs:
- GLSEN offers evidence‑based guidance for inclusive school policies and practices. (See GLSEN resources.)
Gay‑straight alliances, clubs, and peer‑led supports
- Gay‑Straight Alliances (GSAs) and similar student groups reduce isolation, foster belonging, and lower risk for harassment. Schools with active GSAs report improved school climate for LGBTQ+ students.
- Best practices for sustaining groups:
- Secure staff sponsors who are trained and supported.
- Ensure confidentiality and safe meeting spaces.
- Engage in both social support and advocacy activities.
Physical and virtual safe spaces: design and maintenance
- Physical spaces: inclusive signage (pronoun pins, ally stickers), single‑occupancy restrooms, gender-affirming policies for dress codes, and private counseling areas.
- Virtual spaces: moderated forums (e.g., TrevorSpace), clear codes of conduct, and privacy protections.
- Digital safety: teach youth about online privacy, doxxing risks, and safe ways to seek support anonymously when needed.
Transition: Safe environments help prevent crises, but caregivers and allies must recognize warning signs and respond effectively when problems arise.
Practical mental health support for LGBTQ+ youth and families
Identifying warning signs and when to seek professional help
Warning signs that indicate need for professional evaluation:
- Marked changes in mood, prolonged sadness, withdrawal from usual supports.
- Declining school performance, excessive absenteeism, or runaway behavior.
- Self‑harm, suicidal ideation, or talk of hopelessness.
- Substance misuse or risky sexual behaviors used as coping.
If you suspect imminent danger:
- Treat any mention of suicide or self‑harm as urgent. Contact emergency services or a crisis hotline immediately.
- Develop a safety plan and reduce access to means of harm.
“Ask directly about suicidal thoughts — asking does not increase risk and can open the door to support.”
Include routine screening tools in clinics and schools (PHQ‑A for adolescents, GAD‑7 for anxiety), but interpret scores with awareness of minority stress context.
How caregivers and allies can provide immediate support
Communication strategies:
- Listen actively; ask open‑ended questions and reflect feelings.
- Validate experiences: “That sounds painful. Thank you for telling me.”
- Avoid minimizing, dismissing, or pressuring youth to “just get over it.”
Build resilience:
- Encourage social supports, hobbies, and safe peer connections.
- Reinforce protective factors: parental acceptance, school engagement, mentorship.
Connect to care:
- Offer to help find an LGBTQ+ competent provider or accompany youth to appointments.
- Respect autonomy and confidentiality while balancing safety needs; involve emergency services if safety is at immediate risk.
Navigating healthcare systems and confidentiality
Privacy and consent:
- Rules about confidentiality and parental consent vary by country and state/province. In many U.S. states, minors may access certain services (e.g., mental health counseling, STI testing) without parental consent; gender‑affirming medical care often has separate legal frameworks.
- Clinicians should explain confidentiality limits clearly to youth and caregivers at the outset.
Finding competent providers:
- Use directories from The Trevor Project, Gay and Lesbian Medical Association (GLMA), or local LGBTQ+ centers.
- Ask prospective providers about experience with gender-affirming care and affirmative therapy practices.
Overcoming hurdles:
- If insurance denies coverage, seek advocacy through local LGBTQ+ legal organizations or clinics offering sliding-scale services.
- Telehealth can expand access in underserved areas; ensure platforms are secure and private.
Transition: Beyond immediate help, curated resources and tools support ongoing recovery and community building.
Resources for LGBTQ+ teens, allies, and professionals
National and local organizations and hotlines
- Crisis hotlines:
- The Trevor Project Lifeline: 1‑866‑488‑7386 and The Trevor Project (TrevorChat and text 678-678 in some services).
- 988 Suicide & Crisis Lifeline (U.S.): dial 988 — options for LGBTQ+ competent support.
- Trans Lifeline (peer support for trans people):
- Advocacy and support organizations:
- GLSEN — school-based resources.
- Family Acceptance Project — family support research and materials.
- Local LGBTQ+ centers often offer youth groups, counseling referrals, and emergency resources.
When evaluating resources:
- Look for clear statements of cultural competence, trauma‑informed practice, and youth-centered approaches.
- Check whether services are free or low‑cost and available in your region.
Online tools, apps, and educational materials
- Peer support platforms: TrevorSpace, moderated youth forums.
- Mental health apps: evidence-backed apps like CBT-based mood trackers, DBT skill apps, and mindfulness tools (e.g., MindShift CBT, though availability and evidence vary). Always vet privacy policies.
- Curricula and training: GLSEN’s educator resources; professional continuing education modules on gender-affirming care.
- Recommended reading lists: Family Acceptance Project materials, clinician textbooks on affirmative therapy, and trauma‑informed care manuals.
Tailored resources for underserved or intersecting communities
- Racial/ethnic minority supports: seek organizations that explicitly combine racial justice and LGBTQ+ advocacy (e.g., local community centers or national groups with culturally specific programs).
- Rural youth: telehealth platforms, online peer groups, and statewide youth centers can fill gaps.
- Disability-accessible resources: ensure materials are available in multiple formats (audio, large print, captioned videos).
- Language-accessible services: locate providers who offer care in youth’s preferred language or use trained medical interpreters.
Transition: To sustain progress, prevention and evaluation are key components of a system-wide strategy.
Implementing long‑term strategies to support LGBTQ+ youth mental health
Prevention: building resilience and protective factors
Prevention focuses on creating environments that reduce exposure to minority stress and increase protective factors:
- Promote social connectedness through mentorship programs and inclusive extracurriculars.
- Incorporate LGBTQ+ representation into curricula, libraries, and school events.
- Train staff on inclusive practices and restorative approaches to conflict.
- Promote family engagement programs that enhance understanding and acceptance.
Evaluation and continuous improvement of programs
- Monitor outcomes: track attendance, symptom measures, school climate indicators, and rates of bullying incidents.
- Collect youth feedback regularly to adapt services to their needs.
- Use mixed methods (quantitative outcomes plus qualitative youth stories) for a fuller picture.
- Address research gaps: more longitudinal studies are needed on long-term outcomes of affirming interventions across diverse populations.
Advocacy and policy change to reduce systemic inequities
Policy levers:
- Support laws that explicitly protect against discrimination in schools and healthcare.
- Advocate for funding for school counselors and LGBTQ+ community centers.
- Push back against restrictions that block access to gender-affirming care and educational inclusion.
Mobilize stakeholders:
- Build coalitions of youth, families, clinicians, and educators.
- Support youth-led advocacy and ensure young people have leadership roles in policy discussions.
Transition: The path forward requires coordinated, evidence-based, and compassionate action at every level.
Conclusion
Addressing LGBTQ+ youth mental health challenges demands a multi-pronged approach: affirmative therapeutic approaches for LGBTQ+ youth, school and community interventions that focus on safety and belonging, and family work that fosters acceptance. Families, educators, and clinicians all have roles to play — from recognizing warning signs to advocating for policy change.
Practical next steps:
- If you’re a caregiver: start with open conversation, seek family acceptance resources, and connect with local supports.
- If you’re an educator: review school policies, support GSAs, and pursue training in trauma‑informed, inclusive practices.
- If you’re a clinician: adopt affirmative frameworks, screen for minority stress, and build referral networks for gender‑affirming care.
Immediate resources:
- The Trevor Project: — crisis services and youth resources.
- GLSEN educator resources:
- Family Acceptance Project:
- Trans Lifeline:
Example brief safety plan (adapt and personalize):
- Warning signs: (list)
- Coping strategies: (list)
- People/places that help: (names, phone numbers)
- Professional contacts: (clinician, crisis line)
- Steps to make environment safer (remove means): (list)Caring, informed action saves lives. When families, schools, and clinicians collaborate using evidence‑based, trauma‑informed practices, we can reduce harm and help LGBTQ+ youth thrive.
Call to action: Learn one new resource this week, update one policy or practice in your school or clinic, and reach out if a young person needs help — immediate support is available via crisis hotlines and community organizations. To find local supports, visit the national directories linked above or contact your nearest LGBTQ+ center.
Keywords used: understanding LGBTQ+ mental health issues, therapeutic approaches for LGBTQ+ youth, mental health support for LGBTQ+ youth, supporting LGBTQ+ youth in schools, resources for LGBTQ+ teens, LGBTQ+ youth mental health challenges, creating safe spaces for LGBTQ+ teens.
Sources and further reading: